What you'll know after reading this
- The language: Understanding the terminology when it comes to your own
- Some common causes to painful sex and what they mean
- Paths Forward: Treatment and support that feels managable

Pain during sex is common, but it is never something you should simply accept. It can be caused by a wide range of physical, hormonal, psychological and relationship factors, including conditions such as endometriosis, vaginismus, vulvodynia, pelvic floor dysfunction and menopause. Getting the right diagnosis is key, as treatment depends on the underlying cause.
Sex is meant to be pleasurable, fun and something you want to return to without anxiety or fear of pain. But for a lot of women, sex is sadly accompanied by pain, discomfort and even distress. The worst part is, despite being remarkably common amongst those with a vulva/vagina, painful sex remains one of the most under-discussed, isolating and shame-filled topics in sexual health. In fact, many women suffer in silence for years, assuming their experience is just ‘a normal part of sex, unavoidable, or somehow their fault and their body must be ‘broken.’ It is none of these things.
But why do women push through and suffer? Because asking for something else in the bedroom implies we are the broken ones, too much or even undesirable if sex doesn’t look like the movies. Again, you are none of these things.
This article is not only going to help you explore the medical terminology around painful sex but also the many possible causes, and, crucially, the paths forward toward a more comfortable and fulfilling sex life. Because you deserve it, it’s possible, and with the right support, you will get there.
How common is painful sex in women?
First, let’s normalise just how common pain during sex really is, because whether it’s down to something biological, relational or psychological, your pain is real and deserves to be understood. And while it might be common, it doesn’t mean that living with pain around sex is normal.
Research suggests that around 75% of women will experience pain during sex at some point in their lives, and for roughly 10–20%, it is an ongoing, recurring problem.
Yet studies consistently show that women wait an average of four years before seeking help, and many never do at all.
The silence around this issue is partly cultural (sex and pain are both difficult topics to raise with a doctor), partly a result of medical dismissal, and partly because women are so often told that discomfort is “normal” or “just part of being a woman.” It is not. Pain during sex is a signal that something needs support, and it’s worth taking seriously.
The language: Understanding the terminology
Medical terminology can feel clinical and even upsetting at times, but knowing the correct words helps when seeking diagnosis and treatment, especially when it feels like you are being dismissed or referred to the wrong person time and time again.
Dyspareunia is the umbrella term for persistent or recurrent pain associated with intercourse. It can occur before, during, or after sex, and can be felt in different locations, at the vaginal entrance, deep inside the pelvis, or in the vulvar area more broadly. Dyspareunia is classified as superficial (pain at the entrance) or deep (pain felt internally, often in the pelvis or lower abdomen).
Vaginismus refers to involuntary contractions of the muscles surrounding the vaginal opening, making penetration painful, difficult, or impossible. It can be primary (present from the first attempt at penetration, like a tampon or a toy/penis) or secondary (developing after a period of pain-free sex or tampon use). Vaginismus is now understood to exist on a spectrum and is closely connected to both physical and psychological factors.
This one is important! If a doctor does not find any physical issues, vaginismus can also be a result of past trauma or anxiety around penetration. The involuntary muscle response is real and physiological; the experiences or beliefs that may have shaped it are equally real.
Vulvodynia is chronic vulvar pain, like burning, stinging, or rawness of the vulva that has no identifiable cause. It may be localised (for example, vestibulodynia, which affects the vestibule, the tissue at the vaginal entrance) or generalised. Vulvodynia can occur with or without touch, and is frequently misdiagnosed or dismissed.
Genitopelvic pain/penetration disorder (GPPPD) is a more recent diagnostic category from the DSM-5 (the primary reference guide used by mental health and medical professionals) that combines vaginismus and dyspareunia, recognising that the two often overlap and are difficult to distinguish clinically.
Understanding these terms matters more than you might think. Not to reduce your experience to a label, but to give you language to advocate for yourself in medical settings and to help you make sense of what’s going on and how best to support yourself outside the doctor’s room.
Causes of painful sex
Pain during sex can sometimes be down to more than one thing. For example, if you are experiencing a physical issue like Endometriosis, you might find penetration painful, causing the pelvic floor to tighten out of a fear response to pain.
Below is just a quick view of some common causes of painful sex; however, many more reasons also exist outside of this list.
Physical and Gynaecological Causes
Insufficient lubrication is one of the most common and easily addressed causes. Natural lubrication depends on arousal, and many factors can interfere with it, including inadequate foreplay (typically a female would need around 20 minutes), stress, hormonal changes, menopause and certain medications may impact the production of lubrication.
Hormonal changes are a major factor, particularly around menopause, postpartum recovery, and while breastfeeding. Declining oestrogen levels cause the vaginal tissues to thin, dry, and become more fragile, a condition called genitourinary syndrome of menopause (GSM), formerly known as vaginal atrophy. This can make penetration genuinely painful.
Infections, including thrush, bacterial vaginosis, and sexually transmitted infections, can cause inflammation and sensitivity that makes sex uncomfortable.
Skin conditions affecting the vulva, such as lichen sclerosus or lichen planus, can cause significant pain, itching, and tissue fragility.
Endometriosis, a condition in which tissue similar to the uterine lining grows outside the uterus, is a leading cause of deep dyspareunia. Pain during deep penetration, particularly in certain positions, is a hallmark symptom. Yet, Endometriosis takes an average of seven to ten years to diagnose, as symptoms can seem similar to those of other conditions, and treatment can be invasive and expensive.
Pelvic inflammatory disease (PID), ovarian cysts, uterine fibroids, and pelvic floor dysfunction can all contribute to pain during sex. Pelvic floor hypertonicity (excessive tension in the pelvic floor muscles) is increasingly recognised as a significant factor in both dyspareunia and vaginismus.
Childbirth-related trauma, including perineal tears, episiotomies, and scar tissue, can cause pain that persists long after the recommended postpartum waiting period.
Psychological and Relational Factors
The mind and body are not separate when it comes to sexual pain. Anxiety, depression, a history of sexual trauma or abuse, relationship difficulties, and fear of pain itself can all contribute to or amplify physical pain responses.
This is not to say the pain is “all in your head”; it absolutely is not, but psychological factors are real, physiological, and worth addressing alongside physical ones.
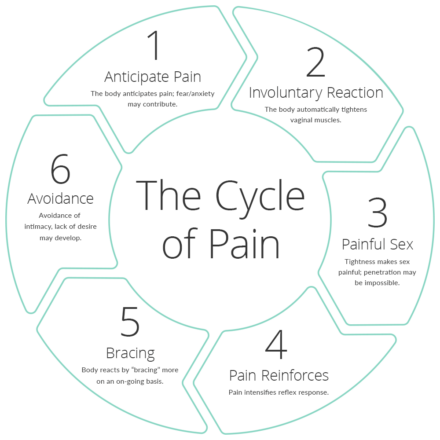
Fear-avoidance cycles are particularly common: pain leads to anticipatory anxiety, which leads to muscle tension and reduced arousal, which leads to more pain. Breaking this cycle is often a central part of treatment. Take a look at the diagram below. This might help you make sense of what’s happening. Working with a trained professional, you can learn ways to support you in breaking away from this.
Paths Forward: Treatment and Support
The good news is that painful sex is not something you have to navigate alone, and often, there are very effective solutions and support. Once the underlying cause is identified, finding the right treatment is just around the corner. Here are a few routes people can take.
I believe the first step is seeing a doctor who takes you seriously. A GP is a starting point, but a gynaecologist, vulvodynia specialist, or sexual health physician or therapist may be more helpful. Be specific about where and when you feel pain (keep a diary), how long it has been happening, and what makes it better or worse. If you feel dismissed, seek a second opinion, a third, and even a fourth until you find the right person for you.
Pelvic floor physiotherapy is one of the most evidence-backed treatments for vaginismus, dyspareunia related to pelvic floor tension, and postpartum pain. A pelvic floor physio can assess muscle tone and coordination, provide hands-on treatment, and guide you through exercises designed to reduce tension and improve function.
Lubricants and moisturisers can make a significant difference for dryness-related pain. While using lube is often seen as taboo, it’s actually something everyone should be using, pain or no pain.
A good place to start is exploring water-based or silicone-based lubricants. Both are used during sex to reduce friction, but make sure you understand what lube you need and what’s safe to use for your body, your sex toys and even on condoms.
Then there are vaginal moisturisers, which are used to help maintain tissue health regularly. Then, finally, there are also options for hormonal changes like the menopause, such as topical oestrogen (low-dose vaginal oestrogen cream or pessaries), which is highly effective and considered safe for most women (always speak with your doctor before using).
Sex therapy and psychosexual counselling address the psychological dimensions of painful sex, including trauma, anxiety, body image, and relationship dynamics. Exploring sex therapy alone or with a partner can be a great tool to invest in while the physical investigations happen. Having a professional who can support your mind and emotions and provide tailored advice and tools to address pain while you explore the root cause can provide an enormous sense of relief and momentum.
Vaginal dilator therapy, often guided by a physiotherapist, uses a graduated series of smooth inserts to gently desensitise the vaginal muscles and rebuild confidence in penetration. It is a cornerstone treatment for vaginismus.
Final words
If you’re experiencing pain during sex, know that you are far from alone, that there are words to describe what you’re going through, an explanation that needs the right investigations, and that effective help does exist.
Your pleasure matters. So does your pain.
Further reading: Pelvic floor therapy: what it is and how it supports pleasure
Sources & further reading.
- The Gynae Centre. Why does sex hurt? 8 Reasons you’re having painful intercourse (Dyspareunia)
- The Pelvic Pain Network. Better care for people living with pelvic pain.
- Lori A. Brotto. Better Sex Through Mindfulness: How Women Can Cultivate Desire
Book a session with April Maria
Embodied Intimacy Coach, Sex Educator & Trainee Psychosexual & Relationships Therapist


